
Vepdegestrant and the Emergence of Targeted Protein Degradation in Breast Cancer
Creators & Contributors


On May 1, 2026, the U.S. Food and Drug Administration (FDA) approved vepdegestrant, marketed as VEPPANU™, for adults with estrogen receptor-positive, human epidermal growth factor receptor 2-negative, ESR1-mutated advanced or metastatic breast cancer, as detected by an FDA-authorized test, after disease progression following at least one line of endocrine therapy [1]. The FDA also approved Guardant360 CDx as a companion diagnostic device to identify patients with breast cancer harboring ESR1 mutations for treatment with vepdegestrant [1]. Arvinas describes VEPPANU™ as the first FDA-approved proteolysis-targeting chimera (PROTAC) therapy [12]. The approval is scientifically important, but it should be interpreted with clinical restraint. The clinical benefit was most evident in the ESR1-mutated population, while the overall trial population did not achieve statistical significance. The lesson is not that catalytic degradation has fixed endocrine resistance. It is that a new pharmacologic approach has reached patients, with a mechanistically coherent and clinically meaningful benefit in a biomarker-defined population, while the magnitude of benefit remains modest.
Endocrine Resistance and the Role of ESR1 Mutations
ESR1 mutations occur in approximately 20–40% of estrogen receptor-positive (ER+) metastatic breast cancers after progression on endocrine therapy, particularly after aromatase inhibitor-based treatment, and are also common in contemporary cohorts previously treated with cyclin-dependent kinase 4/6 (CDK4/6) inhibitors [2], [3]. The most common alterations, Y537S and D538G, in the ligand-binding domain stabilize an active receptor conformation and decrease sensitivity to fulvestrant and some oral selective estrogen receptor degraders (SERDs). Clinically, these mutations are linked to shorter progression-free survival and limited subsequent endocrine options. In this context, later-line endocrine monotherapy often produces short progression-free survival, although outcomes vary by prior endocrine sensitivity, ESR1 mutation status, and trial population. This has driven interest in agents that can achieve deeper and more durable estrogen receptor pathway suppression [4].
Mechanism of Action: From Occupancy to Catalytic Degradation
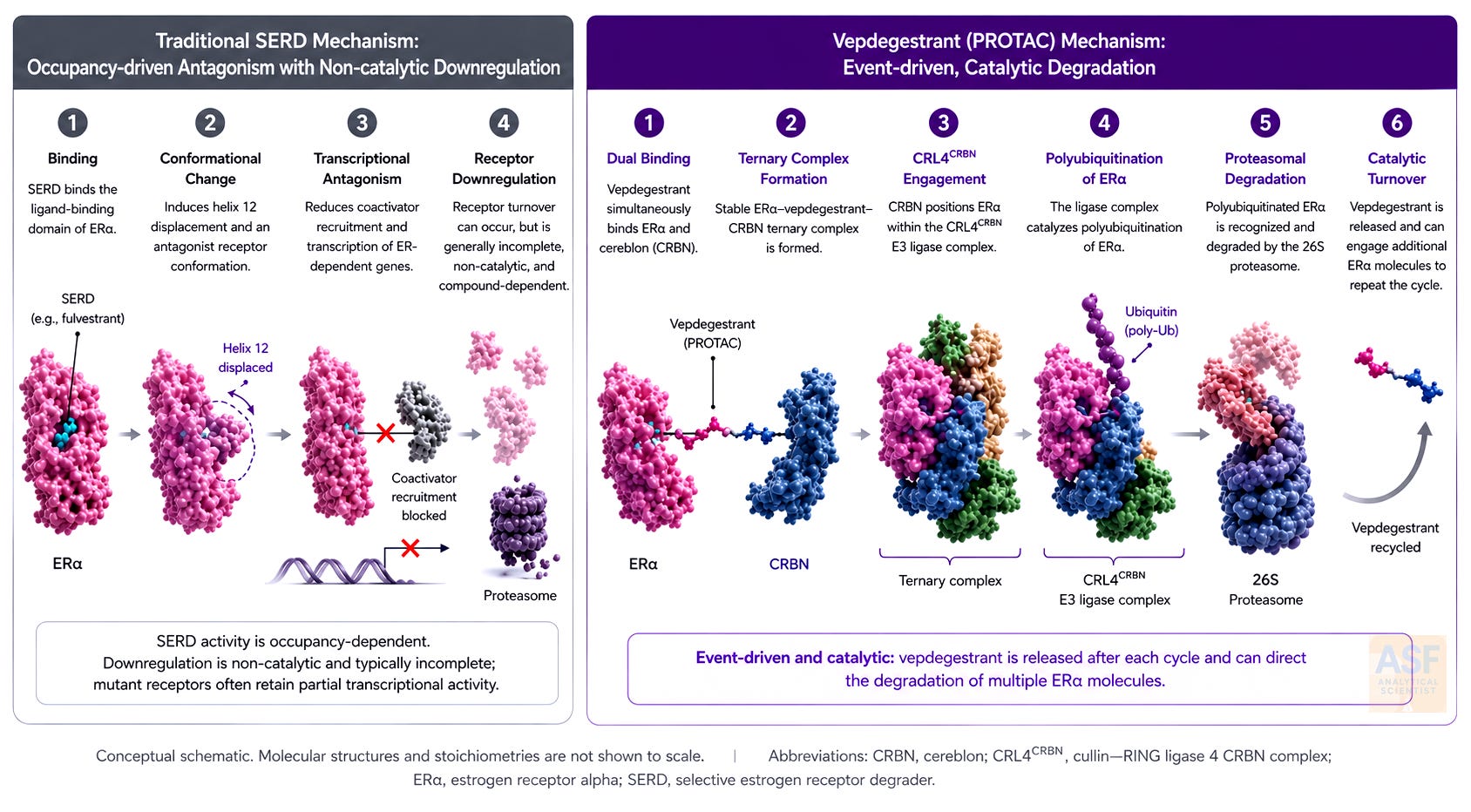
Traditional SERDs operate through occupancy-driven pharmacology. They bind the ligand-binding domain of the estrogen receptor (ER), induce a conformational change that promotes partial proteasomal degradation, and sterically hinder coactivator recruitment. Degradation may remain incomplete, and mutant receptors can retain transcriptional activity. Vepdegestrant operates through an event-driven, catalytic mechanism. It is a heterobifunctional molecule that simultaneously engages the estrogen receptor and the E3 ubiquitin ligase cereblon (CRBN). The resulting ternary complex recruits the CRL4CRBN E3 ubiquitin ligase complex, leading to receptor polyubiquitination and proteasomal degradation. In principle, this event-driven mechanism can allow target degradation without requiring sustained stoichiometric target occupancy, distinguishing PROTAC pharmacology from conventional occupancy-driven inhibition. Preclinical studies reported robust estrogen receptor degradation and antitumor activity in ER-positive breast cancer models, including models with clinically relevant ESR1 mutations, with activity observed as monotherapy and in combination with CDK4/6 or PI3K/mTOR pathway inhibitors [5], [6]. This deeper receptor depletion, rather than receptor occupancy alone, provides a mechanistic rationale for activity in ESR1 mutation-driven resistance.
Analytical Perspectives: Why Degradation Demands More Than Exposure
For an analytical scientist, vepdegestrant demonstrates why targeted degradation cannot be assessed solely from exposure data. For a traditional small-molecule inhibitor, the main question is whether enough drug exposure is achieved at the target for a sufficient period. A PROTAC raises additional questions: whether the compound forms the intended ternary complex, recruits the relevant E3 ligase machinery, induces measurable target degradation, and produces a pharmacodynamic response that correlates with clinical benefit. Exposure, engagement, degradation, and patient selection therefore become interconnected parts of the evidence chain.
Published liquid chromatography–tandem mass spectrometry (LC-MS/MS) methods enabled sensitive measurement of vepdegestrant in rodent plasma. Niessen et al. reported a lower limit of quantification (LLOQ) of 0.5 ng/mL in rat plasma, while Choi et al. reported a validated range of 1 to 1000 ng/mL in mouse and rat plasma [10], [11]. These studies supported preclinical pharmacokinetic and stability assessment, including rodent exposure and matrix-dependent stability behavior. Separately, mechanistic studies supported ER-vepdegestrant-CRBN ternary complex formation and downstream estrogen receptor degradation [5], [6]. Together, these findings illustrate why degrader development requires an evidence chain that links exposure, target engagement, degradation, pharmacodynamic response, and patient selection.
In VERITAC-2, the clinical translation of that evidence chain depended on biomarker selection. ESR1 mutation status was determined using blood-based circulating tumor DNA (ctDNA) through central or local testing, enabling prespecified analysis of the ESR1-mutated population and supporting the companion diagnostic strategy with Guardant360 CDx. That is the broader lesson: for targeted degradation to mature clinically, the field will need rigorous analytics not only for the molecule but also for the target, the degradation event, and the patient population most likely to benefit.
Clinical Validation: The VERITAC-2 Phase 3 Trial
Approval was based on VERITAC-2 (NCT05654623), a global, randomized, open-label Phase 3 trial that enrolled 624 patients with ER+/HER2− advanced or metastatic breast cancer whose disease progressed after one or two lines of endocrine therapy, including at least one CDK4/6 inhibitor-containing regimen [1], [7], [8]. Patients were randomized 1:1 to vepdegestrant 200 mg orally once daily with food or to fulvestrant administered according to standard labeling. Randomization was stratified by ESR1 mutation status, determined by circulating tumor DNA, and by the presence of visceral metastases. Patients had not received prior fulvestrant or chemotherapy for advanced or metastatic disease [1], [7].
In the prespecified ESR1-mutated population (n = 270), blinded independent central review–assessed progression-free survival was significantly longer with vepdegestrant: median 5.0 months (95% confidence interval [CI], 3.7–7.4) versus 2.1 months (95% CI, 1.9–3.5) with fulvestrant (hazard ratio 0.57; 95% CI, 0.42–0.77; P = 0.0001) [1], [7]. Objective response rates were 19% (95% CI, 12–27%) versus 4% (95% CI, 1.6–10%). In the overall population, the difference in progression-free survival did not reach statistical significance (median 3.7 versus 3.6 months; hazard ratio 0.83; 95% CI, 0.68–1.02; P = 0.07). Overall survival data remain immature. The statistically significant progression-free survival (PFS) benefit was observed in the ESR1-mutated subgroup, whereas the overall population did not achieve statistical significance.
The safety profile was manageable but not trivial. The FDA approval summary notes warnings and precautions for QTc interval prolongation and embryo-fetal toxicity [1]. The prescribing information also includes adverse reactions, laboratory abnormalities, dose modification guidance, and clinically relevant interaction considerations involving QT-prolonging drugs, CYP3A inhibitors or inducers, and certain P-gp or UGT1A9 substrates [15]. For a targeted degrader intended for oral chronic use, tolerability, QTc monitoring, and concomitant medication management are not secondary details. They are part of the therapeutic profile.
Therapeutic Landscape and Unresolved Questions
In the EMERALD trial subgroup analysis, elacestrant provided a relevant oral SERD comparison for ESR1-mutated ER-positive, HER2-negative advanced breast cancer [4]. Direct cross-trial comparisons are limited by differences in control arms and eligibility criteria. These differences do not prove that one treatment is superior to the other, but vepdegestrant's fulvestrant-controlled data and degrader mechanism make it a distinct endocrine option. Since VERITAC-2 excluded prior fulvestrant exposure, it does not answer how vepdegestrant performs after fulvestrant or how fulvestrant performs after vepdegestrant. Companion diagnostic testing with Guardant360 CDx supports biomarker-guided patient selection [1]. As noted in expert commentary, the emergence of mechanistically distinct degraders raises important questions about the best sequencing strategies [9].
Several unresolved questions still exist. Resistance mechanisms to PROTACs, possibly involving CRBN downregulation or alterations in ubiquitin-proteasome components, are not fully understood. The optimal sequencing with respect to elacestrant and emerging agents, such as AKT-pathway inhibitors and antibody-drug conjugates, remains uncertain. Real-world adherence, QTc monitoring, concomitant medication management, and long-term safety will require careful post-approval attention. Global disparities in access to circulating tumor DNA testing and the medication itself will influence equitable access to benefits. The median PFS of 5.0 months, representing an absolute difference of 2.9 months compared to fulvestrant, suggests that monotherapy is unlikely to provide long-term disease control for most patients.
Broader Implications
The approval of vepdegestrant marks a significant milestone: the first time a PROTAC has achieved FDA approval and demonstrated meaningful benefit for patients. The event-driven pharmacology of targeted degradation expands what is possible when the therapeutic objective is not merely to inhibit a protein, but to remove it from the cellular system. In breast cancer, future questions will include how ER degraders should be combined with endocrine and targeted therapies, and whether earlier use can provide benefits beyond current biomarker-based strategies. Vepdegestrant provides clinical evidence that CRBN recruitment can be therapeutically effective for an ER degrader in solid-tumor oncology. A broader question for targeted protein degradation is whether clinically useful degrader platforms can expand beyond the heavily used cereblon and von Hippel-Lindau E3 ligase systems.
Recent FDA approvals in breast cancer, including expanded indications for trastuzumab deruxtecan in HER2-positive early-stage disease and datopotamab deruxtecan in unresectable or metastatic triple-negative breast cancer, reinforce a broader shift toward mechanism-defined, biomarker-guided, and modality-diverse treatment. Vepdegestrant belongs in that landscape, but its significance is distinct: it is not another antibody-drug conjugate, but the first approved PROTAC estrogen receptor degrader [13], [14].
Conclusion
Vepdegestrant should be viewed clearly, without hype. It is the first FDA-approved PROTAC, marking a major milestone in targeted protein degradation. It also shows a statistically significant and clinically relevant progression-free survival benefit in ESR1-mutated ER-positive, HER2-negative advanced breast cancer. Nonetheless, median PFS remains measured in months, overall survival data are immature, and the statistically significant progression-free survival benefit was demonstrated in the ESR1-mutated population, not in the overall trial population. That is the clinically important balance: regulatory proof of a new modality, but with a benefit that remains biomarker-dependent and limited in duration. It demonstrates that catalytic degradation can become an approved therapeutic strategy, while reminding the field that mechanism is only the beginning. The future will depend on sequencing, combinations, resistance biology, patient selection, and whether deeper degradation can translate into longer disease control.
References
[1] U.S. Food and Drug Administration, "FDA approves vepdegestrant for ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer," May 1, 2026. [Online]. Available: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-vepdegestrant-er-positive-her2-negative-esr1-mutated-advanced-or-metastatic-breast
[2] N. Chaudhary et al., "CDK4/6i-treated HR+/HER2- breast cancer tumors show higher ESR1 mutation prevalence and more altered genomic landscape," npj Breast Cancer, vol. 10, Art. no. 15, 2024. doi:10.1038/s41523-024-00617-7
[3] L. Boscolo Bielo et al., "Genomic and clinical landscape of metastatic hormone receptors-positive breast cancers carrying ESR1 alterations," ESMO Open, vol. 9, no. 10, Art. no. 103731, 2024. doi:10.1016/j.esmoop.2024.103731
[4] A. Bardia et al., "Elacestrant in ER+, HER2- metastatic breast cancer with ESR1-mutated tumors: Subgroup analyses from the phase III EMERALD trial by prior duration of endocrine therapy plus CDK4/6 inhibitor and in clinical subgroups," Clin. Cancer Res., vol. 30, no. 19, pp. 4299–4309, 2024. doi:10.1158/1078-0432.CCR-24-1073
[5] S. M. Gough et al., "Oral Estrogen Receptor PROTAC Vepdegestrant (ARV-471) Is Highly Efficacious as Monotherapy and in Combination with CDK4/6 or PI3K/mTOR Pathway Inhibitors in Preclinical ER+ Breast Cancer Models," Clin. Cancer Res., vol. 30, no. 16, pp. 3549–3563, 2024. doi:10.1158/1078-0432.CCR-23-3465
[6] C. Tang et al., "Insights Into Vepdegestrant (ARV-471): The First-in-Class Estrogen Receptor Proteolysis-Targeting Chimera Approaching Food and Drug Administration Approval for Breast Cancer," ChemMedChem, vol. 21, no. 6, e202501111, 2026. doi:10.1002/cmdc.202501111
[7] M. Campone et al., "Vepdegestrant, a PROTAC Estrogen Receptor Degrader, in Advanced Breast Cancer," N. Engl. J. Med., vol. 393, no. 6, pp. 556–568, 2025. doi:10.1056/NEJMoa2505725
[8] E. P. Hamilton et al., "Vepdegestrant, a PROTAC estrogen receptor (ER) degrader, vs fulvestrant in ER-positive/human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer: Results of the global, randomized, phase 3 VERITAC-2 study," J. Clin. Oncol., vol. 43, suppl. 17, abstr. LBA1000, 2025. doi:10.1200/JCO.2025.43.17_suppl.LBA1000
[9] P. Neven and S. N. Han, "PROTAC SERD vepdegestrant outperforms fulvestrant for advanced-stage ER+HER2− breast cancer harbouring acquired ESR1 mutations," Nat. Rev. Clin. Oncol., vol. 22, no. 10, pp. 709–710, 2025. doi:10.1038/s41571-025-01062-6
[10] J. Niessen et al., "Development and validation of LC-MS/MS methods for the pharmacokinetic assessment of the PROTACs bavdeglutamide (ARV-110) and vepdegestrant (ARV-471)," J. Pharm. Biomed. Anal., vol. 249, Art. no. 116348, 2024. doi:10.1016/j.jpba.2024.116348
[11] H.-I. Choi et al., "Stability Evaluation and Pharmacokinetic Profiling of Vepdegestrant in Rodents Using Liquid Chromatography–Tandem Mass Spectrometry," Molecules, vol. 29, no. 17, Art. no. 4048, 2024. doi:10.3390/molecules29174048
[12] Arvinas, Inc., "Arvinas Announces FDA Approval of VEPPANU (vepdegestrant) for the Treatment of ESR1m, ER+/HER2- Advanced Breast Cancer," May 1, 2026. [Online]. Available: https://ir.arvinas.com/news-releases/news-release-details/arvinas-announces-fda-approval-veppanu-vepdegestrant-treatment
[13] U.S. Food and Drug Administration, "FDA approves two separate indications for fam-trastuzumab deruxtecan-nxki in HER2-positive early-stage breast cancer," May 15, 2026. [Online]. Available: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-two-separate-indications-fam-trastuzumab-deruxtecan-nxki-her2-positive-early-stage
[14] U.S. Food and Drug Administration, "FDA approves datopotamab deruxtecan-dlnk for unresectable or metastatic triple-negative breast cancer," May 22, 2026. [Online]. Available: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-datopotamab-deruxtecan-dlnk-unresectable-or-metastatic-triple-negative-breast-cancer
[15] U.S. National Library of Medicine, "VEPPANU (vepdegestrant) tablets, prescribing information," DailyMed, revised May 2026. [Online]. Available: https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=751e18d5-1d41-4b67-b1f3-10272ca5312d
Additional details
Description
The first FDA-approved PROTAC proves catalytic degradation can become medicine, but its modest, biomarker-defined benefit shows that mechanism is only the beginning
Identifiers
- GUID
- 197903497
- URL
- https://abrahamfinny.substack.com/p/vepdegestrant-and-the-emergence-of
Dates
- Issued
-
2026-05-26T04:27:59
- Updated
-
2026-05-26T04:27:59
References
- Unknown title https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-vepdegestrant-er-positive-her2-negative-esr1-mutated-advanced-or-metastatic-breast
- Chaudhary, N., Chibly, A. M., Collier, A., Martinalbo, J., Perez-Moreno, P., Moore, H. M., Luhn, P., Metcalfe, C., & Hafner, M. (2024). CDK4/6i-treated HR+/HER2- breast cancer tumors show higher ESR1 mutation prevalence and more altered genomic landscape. Npj Breast Cancer, 10(1). https://doi.org/10.1038/s41523-024-00617-7
- Boscolo Bielo, L., Guerini Rocco, E., Trapani, D., Zagami, P., Taurelli Salimbeni, B., Esposito, A., Belli, C., Crimini, E., Venetis, K., Munzone, E., Fusco, N., Criscitiello, C., Marra, A., & Curigliano, G. (2024). Genomic and clinical landscape of metastatic hormone receptors-positive breast cancers carrying ESR1 alterations. ESMO Open, 9(10), 103731. https://doi.org/10.1016/j.esmoop.2024.103731
- Bardia, A., Cortés, J., Bidard, F.-C., Neven, P., Garcia-Sáenz, J., Aftimos, P., O'Shaughnessy, J., Lu, J., Tonini, G., Scartoni, S., Paoli, A., Binaschi, M., Wasserman, T., & Kaklamani, V. (2024). Elacestrant in ER+, HER2− Metastatic Breast Cancer with ESR1 -Mutated Tumors: Subgroup Analyses from the Phase III EMERALD Trial by Prior Duration of Endocrine Therapy plus CDK4/6 Inhibitor and in Clinical Subgroups. Clinical Cancer Research, 30(19), 4299–4309. https://doi.org/10.1158/1078-0432.ccr-24-1073
- Gough, S. M., Flanagan, J. J., Teh, J., Andreoli, M., Rousseau, E., Pannone, M., Bookbinder, M., Willard, R., Davenport, K., Bortolon, E., Cadelina, G., Gordon, D., Pizzano, J., Macaluso, J., Soto, L., Corradi, J., Digianantonio, K., Drulyte, I., Morgan, A., … Taylor, I. C. (2024). Oral Estrogen Receptor PROTAC Vepdegestrant (ARV-471) Is Highly Efficacious as Monotherapy and in Combination with CDK4/6 or PI3K/mTOR Pathway Inhibitors in Preclinical ER+ Breast Cancer Models. Clinical Cancer Research, 30(16), 3549–3563. https://doi.org/10.1158/1078-0432.ccr-23-3465
- Tang, C., Tian, B., Zhang, B., Zhang, Y., Ke, C., Chen, M., Wei, M., Wang, W., Deng, X., Zhang, Q., Wang, M., Xia, J., He, M., Liang, C., & Tian, L. (2026). Insights Into Vepdegestrant (ARV‐471): The First‐in‐Class Estrogen Receptor Proteolysis‐Targeting Chimera Approaching Food and Drug Administration Approval for Breast Cancer. ChemMedChem, 21(6). https://doi.org/10.1002/cmdc.202501111
- Campone, M., De Laurentiis, M., Jhaveri, K., Hu, X., Ladoire, S., Patsouris, A., Zamagni, C., Cui, J., Cazzaniga, M., Cil, T., Jerzak, K. J., Fuentes, C., Yoshinami, T., Rodriguez-Lescure, A., Sezer, A., Fontana, A., Guarneri, V., Molckovsky, A., Mouret-Reynier, M.-A., … Hamilton, E. P. (2025). Vepdegestrant, a PROTAC Estrogen Receptor Degrader, in Advanced Breast Cancer. New England Journal of Medicine, 393(6), 556–568. https://doi.org/10.1056/nejmoa2505725
- Hamilton, E. P., De Laurentiis, M., Jhaveri, K. L., Hu, X., Ladoire, S., Patsouris, A., Zamagni, C., Cui, J., Cazzaniga, M., Cil, T., Jerzak, K. J., Fuentes, C. S., Yoshinami, T., Rodríguez-Lescure, Á., Valota, O., Lu, D. R., Martignoni, M., Parameswaran, J., Zhi, X., & Campone, M. (2025). Vepdegestrant, a PROTAC estrogen receptor (ER) degrader, vs fulvestrant in ER-positive/human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer: Results of the global, randomized, phase 3 VERITAC-2 study. Journal of Clinical Oncology, 43(17_suppl). https://doi.org/10.1200/jco.2025.43.17_suppl.lba1000
- Neven, P., & Han, S. N. (2025). PROTAC SERD vepdegestrant outperforms fulvestrant for advanced-stage ER+HER2− breast cancer harbouring acquired ESR1 mutations. Nature Reviews Clinical Oncology, 22(10), 709–710. https://doi.org/10.1038/s41571-025-01062-6
- Niessen, J., Nilsson, J. M., Peters, K., Indulkar, A., Borchardt, T., Koziolek, M., Lennernäs, H., Dahlgren, D., & Hedeland, M. (2024). Development and validation of LC-MS/MS methods for the pharmacokinetic assessment of the PROTACs bavdeglutamide (ARV-110) and vepdegestrant (ARV-471). Journal of Pharmaceutical and Biomedical Analysis, 249, 116348. https://doi.org/10.1016/j.jpba.2024.116348
- Choi, H.-I., Choi, J., Kim, J. W., Lee, Y. H., Cho, K. H., & Koo, T.-S. (2024). Stability Evaluation and Pharmacokinetic Profiling of Vepdegestrant in Rodents Using Liquid Chromatography–Tandem Mass Spectrometry. Molecules, 29(17), 4048. https://doi.org/10.3390/molecules29174048
- Unknown title https://ir.arvinas.com/news-releases/news-release-details/arvinas-announces-fda-approval-veppanu-vepdegestrant-treatment
- Unknown title https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-two-separate-indications-fam-trastuzumab-deruxtecan-nxki-her2-positive-early-stage
- Unknown title https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-datopotamab-deruxtecan-dlnk-unresectable-or-metastatic-triple-negative-breast-cancer
- Unknown title https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=751e18d5-1d41-4b67-b1f3-10272ca5312d